
Flat Head Syndrome: When to Worry & What to Do
By Melissa McDougall, Advanced Paediatric Osteopath (as awarded by Osteopathy Australia in 2021)
As a parent, searching for answers, you may have recently noticed or recently been told that your baby has flat head syndrome, otherwise known as positional plagiocephaly. This can be a concern for parents, as we all want our babies to grow and develop in a balanced and healthy way.
Flat head syndrome is a common occurrence in babies. A Review of the Research in 2022 states that flat head syndrome, or Positional Plagiocephaly/Deformational Brachycephaly has increased from 0.3% to 48%, after the introduction of the Back to Sleep Campaign (a wonderful campaign that has saved many infant lives from SIDS). So know that you, and your baby, are not alone.
The good news is it can be treated by getting the right advice and support early. I’ll stress this point- the earlier you get help, the better! This article can serve as your first line of help. Flat head syndrome can also be prevented, so if you are pregnant, or your baby does not have a flat head yet– keep reading!
In this article you will learn:
👶🏼 What is Flat head Syndrome and Why Does it Occur
👶🏻 How to Know if Your Baby is at Risk of Developing a Flat Head
👶🏾 Prevention of Flat Spots
👶🏽 Treatment for Flat Spots
👶🏼 Is Flat Head Syndrome Just an Aesthetic Problem?
👶🏻 Baby Flat Head, When to Worry
👶🏾 What You Can to TODAY to Help Your Baby
What is Plagiocephaly or Flat Head Syndrome?
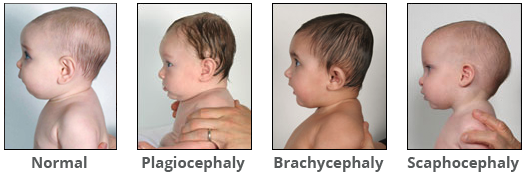
Plagiocephaly and brachycephaly are two of the most common types of flat head syndrome, affecting 48% of babies. The two conditions describe very different head shapes, and in my osteopathic experience, these differences are associated with different patterns of muscle tightness in the body. This means the treatment for each is also different.
Signs and Symptoms of Flat Head Syndrome
Plagiocephaly is the term to describe an asymmetrical head shape with a flattening to one side of the head. With mild plagiocephaly, if you look at the back of your baby’s head, you may notice that your baby has only a slight flattening of one side. With moderate to severe plagiocephaly, ear shift and other facial changes occur as the head moves into a parallelogram shape. You may notice that one of your baby’s eyes looks bigger, or higher than the other, one ear sticks out more, and their forehead on the same side as the flattening is more prominent. You may also notice mouth or jaw deviation to one side.
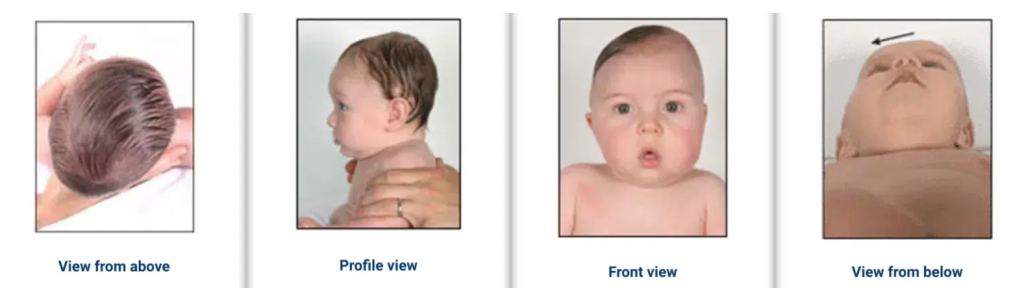
Compensatory changes occur because your baby’s skull is soft and deforms to maintain the same volume for the growing brain- which we definitely want!
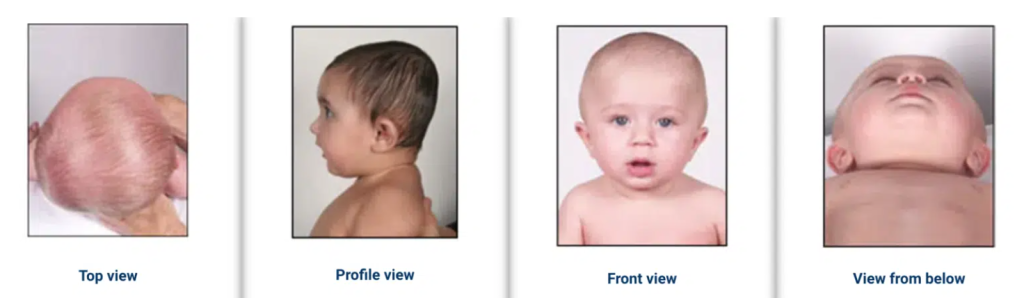
Brachycephaly is the term to describe symmetrical flattening of the back of the head, severity can also range from mild to severe. With mild brachycephaly, you may notice a slight central flattening of the back of your baby’s head. With more severe brachycephaly, you will notice your baby’s head seems wide and face can be ‘full moon’ shaped, but there is usually very little change in face symmetry.
Compensatory changes occur again because your baby’s skull is soft and deforms to maintain the same volume for the growing brain.
To understand the differences, look at the below comparisons:

What Causes Flat Head Syndrome?
Newborn flat head and flat head syndrome in older babies usually (but not always) results from one, or a combination of three things:
👶🏾 Your baby’s position during pregnancy
👶🏼 Pressure on your baby’s skull, and strain on their neck muscles during birth
👶🏻 A preference for your baby to position their body and head in a certain way after birth. For example – only turning their head one way when lying on their back.
It is normal and helpful for a baby’s head to change shape during the birth process, and ‘cone-shaped’ heads or other skull adaptations can resolve quite quickly.
However, if your baby is born with a flat spot and facial asymmetry, this may be caused by your baby lying in one position too long during pregnancy, with their head under your rib cage (if breech) or on your pelvic bone (if head down). This sometimes happens to babies that don’t move much in utero, when there is low amniotic fluid or they are big for their gestational age.
By far the most common cause of flat head syndrome is postural preferences after birth. Babies usually sleep a lot (sorry if your baby doesn’t!). They also spend a lot of time in prams- on their back, capsules and in car seats (slightly inclined on their back) on the floor (on their back as tummy time is tricky for long periods) on their back to sleep. The longer your baby prefers to turn their head one way, the more pressure is applied to that side of their head and that’s how flat spots develop in babies with asymmetrical flattening (plagiocephaly).
Babies with symmetrical flattening (brachycephaly) also have a postural preference- however in these cases they don’t turn their head either way to sleep (or they turn very little, not all the way). They often have tight muscles on both sides of their neck, and this pushes the back of their head more firmly into the mattress, floor or other surface they are lying on.
How is Flat Head Syndrome Diagnosed?
The degree of flattening, or severity of flattening in plagiocephaly can be measured in two ways.
1. Cranial Vault Asymmetry Index (CVAI)
CVAI is measured with callipers or 3D scanning. Callipers are proven to be useful in identifying flat head syndrome, and we use these in our clinic to measure the ratios of the skull and work out the severity of asymmetry. This, as well as your baby’s age, informs our treatment plan. Diagonal measurements of the skull are taken and put into an equation to work out the Cranial Vault Asymmetry Index (CVAI).

The equation is (DA-DB) X 100 / DA or DB (whichever is higher)
These measurements are shown by green lines in the image below.

CVAI measurements grade severity on a scale of 0-5. A CVAI score below 3.5 reflects symmetry within normal limits, a CVAI score above 11 reflects severe asymmetry with forehead and facial changes described above.
Some cranial orthotic (helmet) clinics use 3D light scanning to measure CVAI.
CVAI is only accurate with callipers if the asymmetry extends above the ear where the measurements are taken. In my experience, some babies can have flattening much lower and changes to ear position and facial symmetry, but their CVAI measured with callipers is normal. In these cases, we need to use another classification system, described in the next section.
Brachycephaly severity can also be measured with callipers or 3D scanning using the Cranial Index (CI). The equation is cranial width (or biparietal diameter) / cranial length (or occipitofrontal diameter) x 100. A CI above 90 reflects brachycephaly. These measurements are shown by blue lines in the image above.
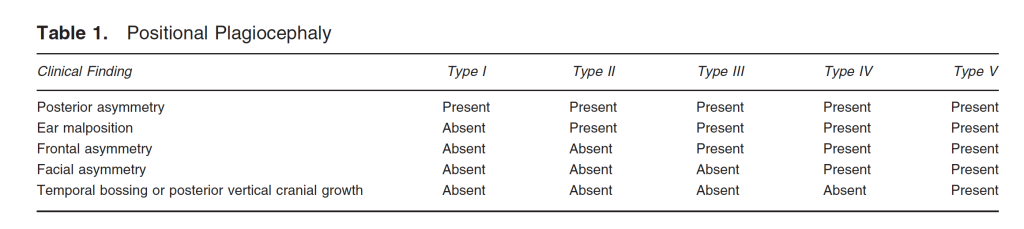
2. Argenta’s Clinical Classification or Plagiocephaly.
Argenta’s classification system is purely observational and can be performed easily by anyone with attention to detail, including parents – although it is much easier for someone like me or my team of Paediatric Osteopaths (if you’re in Melbourne) or another health professional who works with newborn flat head syndrome every day.
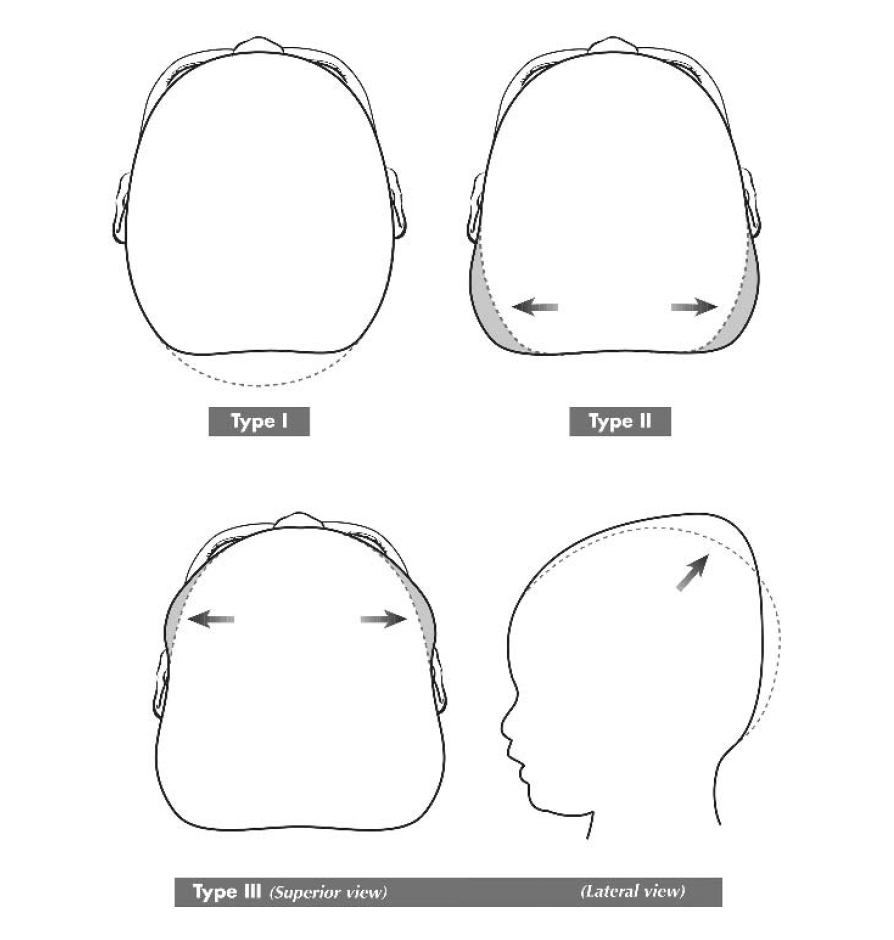
The classification is outlined below. As you can see, there are 5 stages of occipital plagiocephaly progressing from minimal to severe deformity.
Type I deformity is restricted to the back of the skull
Type II adds malposition of the affected ear
Type III adds forehead deformity
Type IV adds malar (cheek) deformity
Type V adds attempts of the brain to decompress vertically (longer head) or temporally (wider head)
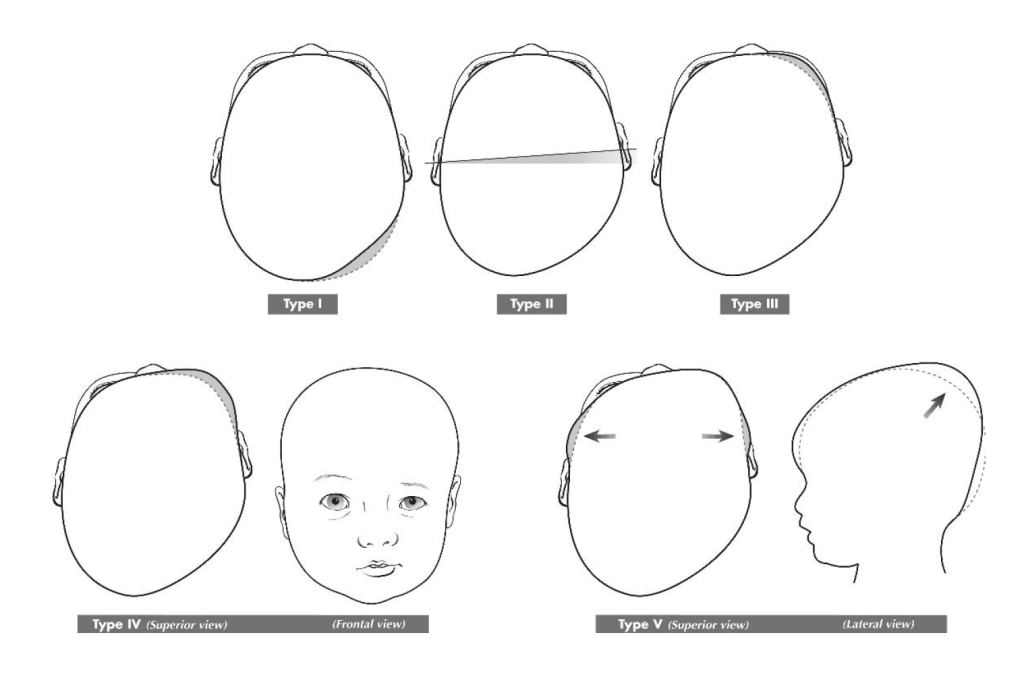
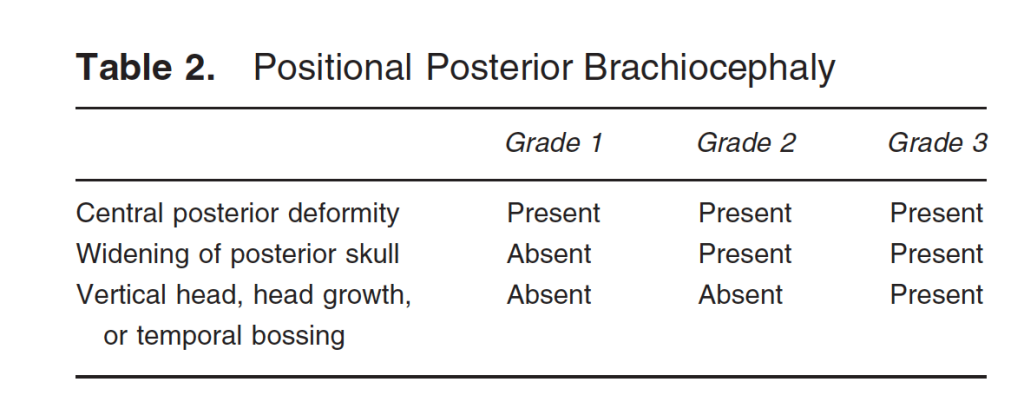
The classification can also be used to identify brachycephaly. There are only 3 stages of posterior brachycephaly.
Type I is restricted to the central posterior skull.
Type II demonstrates widening of the posterior skull lateral to the central depression.
Type III represents attempts to decompress the brain with temporal (wide) or vertical (long) skull growth.
Treatment for Flat Head Syndrome
Repositioning for Newborn Flat Head
The first solution for your baby is repositioning. Usually, your GP, Maternal and Child Health Nurse or Paediatrician will give you ideas about this. Repositioning involves being aware of the way your baby prefers to hold their body or turn their head, and you encourage them to do the opposite. Repositioning can include:
👶🏼 Putting bright and noisy toys on the non-preferred side of the car seat, pram etc.
👶🏻 Position your baby’s cot so that the door or your bed is on their non-preferred side.
👶🏾 Hold your baby in a way that encourages movement to the non-preferred side.
For some babies, repositioning is enough to prevent a flat head developing if it is started early.
Physical Therapy and Exercise for Flat Head Syndrome
If your baby has a flat head, and you are wondering when to worry- If your baby is not responding to repositioning, see an experienced Paediatric Osteopath as soon as possible.
In my experience, a baby fails to respond to repositioning because they can’t move their head a certain way. It’s not comfortable, sometimes not even possible due to muscle strain and postural compression, particularly through the upper neck and base of the skull.
With osteopathic care, parents usually notice an improvement in their baby’s mobility after the first, second or third treatment – however, head shape changes can take longer as the skull needs to grow to change shape.
All of our osteopathic sessions for babies include age-appropriate exercises and activities for home, and these are tailored by experienced professionals for your baby’s needs.
I always recommend getting early support for a flat spot because of the window of opportunity we have to intervene, when a baby is young, due to the great amount of head growth they have in the first 8-12 months of life.
Below is the World Health Organization’s (WHO) head circumference growth charts for boys from 0-2 years (girls charts are very similar).
From these charts let’s reference a boy on the 50% percentile (average). His head growth would average
👶🏻 2.25 cm per month in the first 2 months of life,
👶🏽 1 cm per month between 2 and 6 months old,
👶🏾 0.5 cm per month from 6-10 months old,
👶🏼 and this rate of growth gradually decreases until the age of 2 years.
Ideally, the time to prevent your baby from developing a flat head is to check in with an experienced paediatric osteopath after birth as early as possible. Osteopaths can often pick up slight and early postural preferences that are much easier to resolve early, before any head shape change has begun.
The next best time (if you already notice your baby has a flat spot) is before 8 weeks old. As you can see from the head growth charts, a baby’s head grows very quickly in the first 8 weeks of life, so flat spots can appear quickly- as the skull grows rapidly in all directions except for the spot the baby is always lying on.
The later a baby receives support from a knowledgeable health professional, the more time a flat spot can get worse, and the less time we have to reverse the flat spot while head growth is rapid.
Research suggests the best results for plagiocephaly using manual therapy, including osteopathy are found in babies that present for treatment before 8 weeks old. Again, my advice is don’t wait and see! Get advice and support early.
An exercise example we would sometimes recommend for plagiocephaly (asymmetrical flattening) is below. Baby’s with plagiocephaly may also have a side bending preference or tilt their head or body to the same or opposite side to their flat spot.
You can look through photos of your baby on a flat surface to see if they have a preference to tilt their body or head to one side. The image below shows a baby with a side-bending preference (head tilt) to the right . It’s often helpful to work on a side-bending preference to help resolve head rotation preference.

The image below shows how you can help stretch your baby with a side-bending preference (head tilt) to the right, by holding them right side down.

You can see in the photo above, the baby is very comfortable in this position. If you hold your baby like this, it is important that your baby is comfortable. If not, do not continue and seek advice from your GP, Maternal and Child Health Nurse, Paediatrician or experienced Paediatric Osteopath.
For babies with brachycephaly (symmetrical flattening) muscles on both sides of the front of the neck are usually quite tight. Your baby may seem to have a short neck, their chin down and shoulders raised. Here we want to support your baby to lift their chin. You can do this in a superbaby pose (also great for warming babies up for tummy time). Babies with brachycephaly often dislike tummy time due to the difficulty they have lifting their chin… these exercises may help.

Again, you can see in the photo above, the baby is very comfortable in this position. If you hold your baby like this, it is important that your baby is comfortable. If not, do not continue and seek advice from your GP, Maternal and Child Health Nurse, Paediatrician or experienced Paediatric Osteopath.
These are just a few examples of our recommendations to help your baby move better. For more tailored exercises for your baby, you can access our in clinic appointments, or online support.
Helmet Therapy
Sometimes a baby will need a cranial orthotic (helmet). These have an optimal time frame to be fitted (usually 5-6 months of age) and frequently won’t be offered to babies over 10- 12 months during the slowing of head growth over this age. It is beyond the scope of the article to expand more or helmet therapy, but your Paediatrician, GP or experienced paediatric osteopath will be able to assess your baby and refer you for appropriate care if necessary.
Tips for Preventing or Reducing Flat Head Syndrome
We live in a world full of baby props- bouncers, activity centres, swings, slings, capsules… Often the best things to prevent or reduce flats spots are the most basic: floor time and social play. Here are some of the best, and most inexpensive ways you can prevent or reduce your baby’s flat spot:
Take Vitamin D in Pregnancy and Early Infancy
If you are reading this while pregnant, it’s helpful to check you are getting adequate amounts of vitamin D as maternal deficiencies in this vitamin have been shown to increase this risk of skull deformation in their infants. Similar findings have been demonstrated in young infants- low Vitamin D levels increase the risks of flat spots developing. Always speak to your GP or Paediatrician before supplementing, and ask about the preferred brand of supplement and dose.
Tummy Time
Tummy time on the floor should be started from birth during awake times. Starting tummy time early gets your baby used to the feeling of the front of their body in contact with a hard surface.
Newborns sleep a lot, and it is not unusual for them to fall asleep when you place them on the floor with their head turned to the side. This is OK and normal. If your newborn falls asleep during tummy time, soon transfer them to a safe sleep surface.
The picture below shows Otis at 11 days old on his tummy.

Most babies born around their due date hold their arms and legs bent and close to their body. This is called flexor tone and a sign of a healthy nervous system- however it can make tummy time a bit difficult! You can assist your baby by raising their chest a little higher than their hips by using a rolled towel (see image below).
The photo below shows Otis at 3 months old, using a towel for tummy time support.

Some babies can be quite unsettled during tummy time. For more tummy time tips, read our Advanced Practitioner Guide: Help My Baby Hates Tummy Time
Alternate Your Baby’s Position
It is not just tummy time that is important for head control. In a recent review, Researchers highlight the lack of advice for the prevention of flat spots. Here it is suggested that the focus is on tummy time and face time.
Why?
Tummy time helps your baby build and strengthen their back muscles, and the muscles that extend their neck (look up). But babies also need to strengthen the neck muscles at the front of their neck- these muscles bring their chin to their chest (look down) and working one side at a time, also help turn the head.
From this article, a helpful parent handout was created with some ideas of how you can help your baby strengthen both the back and front of their neck. The idea here is the more quickly your baby can control their head and build their neck strength, the more easily they will be able to move their head and vary their head position to avoid flat spots…. and learn!
This is a great preventative tool for babies, but may be less effective in babies with a very strong preference to lie one way. If you’ve tried these things and still your baby only positions themself one way, or seems uncomfortable when you encourage them to move a different way – see your GP, Paediatrician or experienced Paediatric Osteopath as soon as possible. If you don’t have an osteopath close by, sign up for our online support.
Vary Carrying Positions
When you visit our clinic to seek support for your baby’s head shape, we ask you to reflect on the ways they hold, feed and settle your baby. Adults generally have a dominant hand and find it more comfortable to handle their baby in a certain way- normal!
The idea here is to review the ways you (and other primary caregivers) handle your baby- holding, feeding, settling – and vary these. For example, if your baby breastfeeds in a cradle hold on the left breast, and a football hold on the right, this means your baby isn’t changing their feeding position- they are right side down, slightly looking left.
Or if you and your partner both hold your baby in your left arm to bottle feed- again, your baby isn’t changing their feeding position- they have the right side of their head against you and they are slightly looking left.
Note: If your baby is having feeding difficulty, you may need to do whatever works- also ensure you seek support from a qualified and experienced Lactation Consultant (often they can also help with bottle feeding).
Aside from feeding, there are other positions that both parents can review to ensure they are varying carrying positions:
👶🏻 Which shoulder do you hold your newborn over?
👶🏼 Which arm do you hold your baby in (cradle hold)?
Caregivers should compare the ways they hold their baby and where possible vary feeding and settling positions. Sometimes this is not possible due to personal injury, or differences in coordination or strength- in this case, hold your baby in a way you feel most stable and secure (even if this is only one way). You can still focus on the other tips I share here.
Limit Time in Car Seats and Bouncers
Your baby learns everything first through movement. The best way to help your baby learn is by allowing for more time for face time and tummy time during the day- this means limiting the time your baby spends with their body and back of head supported in car seats, capsules, bouncers or other devices.
Car seats, capsules, and bouncers apply pressure to the back of your baby’s head, and if your baby prefers to lie or look one way, the pressure will be on one side of the back of their head… and you guessed it- predispose to a flat spot developing or worsening.
Time in car seats, capsules, bouncers and other devices also reduces the time your baby has to develop their neck/back strength and gross motor skills like rolling, pressing up off the floor and later reaching and crawling.
The best things in (your baby’s) life are free! Spend time on the floor for your baby’s body and play with them for their mental wellbeing.
Encourage Motor Skills
If you are reading this and have a very unsettled baby that doesn’t enjoy anything – I haven’t forgotten you!
In his book Building Healthy Minds, Dr. Stanley Greenspan shares that the first thing a baby needs to learn is to become calm and interested in the world- and I couldn’t agree more!
When you bring your unsettled baby to our clinic, the first thing we do (before working on anything else) is help you with settling techniques. It is beyond the scope of this article to discuss infant unsettledness – but I can share two general tips for helping your baby through the early weeks… they are movement and white noise. You can try walking around with your baby facing tummy down over your arm.

The sound of a rainmaker can also be a wonderful distraction and soothing for newborns. Rainmakers are also available to purchase from our clinic.
If you have tried these things and still your baby is very unsettled see your GP, Paediatrician or experienced Paediatric Osteopath as soon as possible. If you don’t have an osteopath close by, sign up for our online support for more settling tips.
Once your baby is more settled, you can work on the types of play outlined here to encourage general motor skills development. With independent movement and motor skills comes the ability to move off a flat spot and resolution of postural preferences.
Use of a Baby Carrier
A baby carrier can help distribute your baby’s weight more evenly and reduce pressure on the skull when used correctly. See Raising Children’s helpful guide on baby carriers, safety and healthy hip positioning and the T.I.C.K.S. rule to help you remember how to position your baby safely in a baby sling: Tight; In view at all times; Close enough to kiss; Keep chin off the chest; Supported back.
Baby carriers are not created equal. Most carriers on the market today are designed with hip health in mind, but older designs (that may be handed down to you) are not. It is beyond the scope of this article to expand on our recommendations, but look for a design that allows your baby to get into a M position- knees higher than bottom.
A pelvic tuck can help you position your baby’s hips correctly (in a carrier designed for hip health). If your baby does not settle into a carrier straight away- go for a walk outside- a breeze, white noise of traffic and the movement of walking often will help your baby settle.
When to Seek Professional Help
It’s important to note that this article describes positional flat head syndrome. There are other, more serious causes of cranial asymmetry. If your baby has a flat head, when to worry – see your GP or Paediatrician if any of the following are present:
👶🏼 The skull and facial asymmetry may be more severe than described and pictured above. This can be due to early fusion of one or more cranial sutures (craniosynostosis). An experienced paediatric osteopath may also help identify non-positional causes of plagiocephaly and refer you to appropriate care.
👶🏽 Developmental delay of gross motor, fine motor, social, visual or auditory milestones. An experienced paediatric osteopath may also help identify developmental delay and refer you to appropriate care.
👶🏻 a strong preference for turning their head to one side
👶🏼 difficulty turning their head left or right.
The Role of an Osteopath in Managing Flat Head Syndrome
An osteopathic assessment at Growing Bones includes a full case history, and thorough physical examination of your baby by a Senior Paediatric Osteopath, with more than 10 year’s experience.
The osteopath will then explain the factors that are thought to be contributing to postural preference and explain the treatment plan. Osteopathic treatment for babies involves holding and moving your baby in different ways, using no more pressure than you would when holding or dressing, with the aim of reducing postural preferences, improving mobility and keeping your baby calm and comfortable throughout.
Your osteopath will re-measure your baby’s head every 2-4 weeks, depending on their head growth to monitor or change your treatment plan.
All of our osteopathic sessions for babies include take-home exercises, activities and advice, and these are tailored by professionals for your baby’s needs.
If you don’t have an experienced Paediatric Osteopath nearby, you can sign up for our online support. We have found that when parents continue holding and moving their babies between visits to our clinic, results are seen much quicker. With our online support, we offer a simple way to help your baby at home. We will help you discover activities that promote comfort, freedom of movement and learning- all essential for preventing or reducing flat head syndrome!
Does Flat Head Syndrome Go Away?
In the past, many parents were assured their baby’s flat spot would ‘fix itself’ once their baby starts moving. This advice is still out there, but more and more infants are referred for osteopathic support early. Early support is required when a baby has a strong postural preference – for example looking one way, that is not improving with general advice and repositioning.
Your baby’s nervous system is not ready for independent, controlled movement for months after birth. This means your baby spends most of their time lying down, or held, with their body positioned in a way that is most comfortable for them. I hear this a lot after repositioning fails- you may be trying EVERYTHING to encourage your baby to turn their head to their non-preferred side- but they won’t. This doesn’t mean your baby ‘just likes’ their preferred side- it means they physically cannot move any other way- they have muscle or postural tension that prevents free movement…. this is when they need help.
So does flat head syndrome go away without treatment? In my experience, Yes and No.
Yes, Flat Head Syndrome can fix itself, without treatment when
✅ the cause is positional and
✅ your baby can move in a free and balanced way and
✅ your baby enjoys tummy time and face time play and
✅ the flat spot is mild and
✅ any head preference has resolved by 2 months, or 8 weeks of age.
On the other hand, there are older school-aged children with flats spots that didn’t resolve on their own! So in my experience, Flat head syndrome doesn’t fix itself without treatment when
❌ the cause is positional but your baby cannot move in a free and balanced way
❌ your baby has a strong preference to turn their head one side
❌ your baby sleeps for long periods with their head in one preferred position (more than 70% of the time)
❌ your baby dislikes tummy time and face time play (limiting opportunities for independent movement and getting off the flat spot!)
❌ the flat spot is moderate or severe
❌ the cause is not positional
Another question parents ask is if flat head syndrome is purely aesthetic- that is does it affect learning and development or predispose to other health issues?
Plagiocephaly does not usually affect the development of a baby’s brain, but if left untreated it may change their physical appearance by causing uneven growth of their face and head.
A longitudinal (long term) study in 2011 compared the development of 227 with plagiocephaly (Flat Head Syndrome) with 232 children without head shape change. At 18 months old, the toddlers with plagiocephaly scored lower than children without head shape change, with the largest differences noted in cognitive and language skills, and smaller differences noted in motor skills. Despite the differences between the groups, most children in the study scored within the typical range for their age and above the level to be medically diagnosed with developmental delay.
Positional Plagiocephaly or Brachycephaly develops because of a limited ability to move in a free and balanced way. Limited movement can result in missed opportunities for learning through play as an infant- but from the research, these delays don’t usually result in clinically significant developmental delay.
Helping your child move better, so they can learn better in infancy (and of course improve their flat spot) is a great investment in your time.
Secure Your Peace of Mind & Consult with a Paediatric Osteopath
So in summary,
✅ Flat Head Syndrome is very common in babies and can resolve with the right advice and support.
✅ Look for postural preferences early and seek medical advice early (before your baby is 8 weeks old) – Don’t wait and see.
✅ Enjoy tummy time and face time activities with your baby from day 1 for healthy head control and learning opportunities to help prevent flat spots.
✅ Find the right medical professional and advocate for your child- get a second opinion if the advice doesn’t feel right. You often know your child better than anyone.
You’ve done your baby a great service by taking the time to educate yourself and read this blog, it has been researched at length and written with care and experience. My aim is to help your baby move better from day 1… and have a lovely round head!
If you are local in Melbourne (we’re located in Yarraville), we would love to see you and your baby in our clinic. You are welcome to book an appointment if you have any concerns about your baby’s head shape. If you live further, you can explore our online support options.
This article has been written by Melissa McDougall, Advanced Paediatric Osteopath (as awarded by Osteopathy Australia in 2021), an Osteopath with extensive experience and practice focus in paediatric osteopathy. The information contained in this article is intended as general information about conditions and treatment options which may assist, not replace, discussion with your doctor or health care professional. You should seek specific advice about your own, or you child’s condition, from a health care professional who is able to conduct an examination of the patient’s condition. Melissa McDougall and Growing Bones PTY LTD (and any other authors who post information on this blog) do not accept any responsibility, and will not be liable for the information in this article, any inaccuracies or omissions within the information or for any loss suffered by a person relying on this information. The author(s) and publisher do not represent that the treatment regimen detailed in this article will be successful or appropriate for any particular patient.
Copyright © 2023, Melissa McDougall, Growing Bones PTY LTD.
References
Argenta, L., David, L., & Thompson, J. (2004). Clinical classification of positional plagiocephaly. The Journal of craniofacial surgery, 15(3), 368–372. https://doi.org/10.1097/00001665-200405000-00004
Baby Bunting (n.d.) ELC rainmaker. Retrieved August 1, 2023, from https://www.babybunting.com.au/product/elc-rainmaker-93815?istCompanyId=e136afe6-fe62-489b-abc8-c9de17deb6b8&istFeedId=82d466cf-4ae1-474b-8ca8-9866c775bb45&istItemId=pimilrmtr&istBid=t&cq_src=google_ads&cq_cmp=18314104975&cq_con=&cq_term=&cq_med=pla&cq_plac=&cq_net=x&cq_pos=&cq_plt=gdp&gclid=Cj0KCQjwn_OlBhDhARIsAG2y6zP-U0HnTrkvDLLI3rJ-Bv5fU8CZeiBAu8chgDE9JJ13d_QrOjw1aHYaAmh3EALw_wcB
Children’s Healthcare of Atlanta. (2015). Plagiocephaly Severity Scale. Retrieved August 1, 2023, from https://pediatricapta.org/special-interest-groups/HB/ORTH_961942_PlagiocephalyScale_BWInfo.pdf
Department of Plastic and Maxillofacial Surgery, Royal Children’s Hospital. (n.d.) Information for health professionals: Deformational Plagiocephaly. Retrieved August 1, 2023, from https://www.rch.org.au/uploadedFiles/Main/Content/plastic/Deformational_Plagiocephaly.pdf
ErgobabyUKIreland. (n.d). Pelvic Tuck. Retrieved August 1, 2023, from https://www.youtube.com/shorts/0OGRGk8M67A
Filisetti, M., Cattarelli, D., & Bonomi, S. (2020). Positional plagiocephaly from structure to function: Clinical experience of the service of pediatric osteopathy in Italy. Early human development, 146, 105028. https://doi.org/10.1016/j.earlhumdev.2020.105028
Greenspan, S. (2000). Building Healthy Minds: The six experiences that create intelligence and emotional growth in babies and young children. DaCarpo Press.
Inchingolo, A. D., Inchingolo, A. M., Piras, F., Malcangi, G., Patano, A., Di Pede, C., Netti, A., et al. (2022). A Systematic Review of Positional Plagiocephaly Prevention Methods for Patients in Development. Applied Sciences, 12(21), 11172. MDPI AG. Retrieved from http://dx.doi.org/10.3390/app122111172
International Hip Dysplasia Institute. (2023). Baby Wearing. Retrieved August 1, 2023, from https://hipdysplasia.org/baby-wearing/
Lactation Consultants of Australia and New Zealand (LCANZ). 2023. Find a Lactation Consultant. Retrieved August 1, 2023, from https://www.lcanz.org/find-a-lactation-consultant/
Maedomari, T., Miyabayashi, H., Tanaka, Y., Mukai, C., Nakanomori, A., Saito, K., Kato, R., et al. (2023). Cranial Shape Measurements Obtained Using a Caliper and Elastic Bands Are Useful for Brachycephaly and Deformational Plagiocephaly Screening. Journal of Clinical Medicine, 12(8), 2787. MDPI AG. Retrieved from http://dx.doi.org/10.3390/jcm12082787
Raisingchildren.net.au. (n.d.) Baby carriers, slings and backpacks: safety guide. Retrieved August 1, 2023, from https://raisingchildren.net.au/newborns/safety/equipment-furniture/baby-carrier-sling-safety
Raisingchildren.net.au. (n.d.). Plagiocephaly. Retrieved August 1. 2023, from https://raisingchildren.net.au/newborns/health-daily-care/health-concerns/plagiocephaly#:~:text=See%20your%20GP%20or%20child,their%20head%20left%20or%20right
Red Nose. National Scientific Advisory Group (NSAG). (2016). Information Statement: Why Back to Sleep is the Safest Position for Your Baby. Retrieved August 1, 2023, from https://rednose.org.au/article/why-back-to-sleep-is-the-safest-position-for-your-baby
The Royal Children’s Hospital (RCH). 2017. Baby’s Head Shape: Face time and tummy time equals head control. Retrieved August 1, 2023, from https://www.rch.org.au/uploadedFiles/Main/Content/physio/Head%20control%20fact%20sheet.pdf
The Royal Children’s Hospital Plastic and Maxillofacial Surgery, General Medicine, Physiotherapy and Orthotics departments with the University of Melbourne. (2020). Plagiocephaly. Retrieved August 1, 2023, from https://www.rch.org.au/kidsinfo/fact_sheets/plagiocephaly_misshapen_head/#:~:text=Deformational%20plagiocephaly%2C%20also%20known%20as,of%20their%20face%20and%20head.
van Vlimmeren, L. A., van der Graaf, Y., Boere-Boonekamp, M. M., L’Hoir, M. P., Helders, P. J., & Engelbert, R. H. (2008). Effect of pediatric physical therapy on deformational plagiocephaly in children with positional preference: a randomized controlled trial. Archives of pediatrics & adolescent medicine, 162(8), 712–718. https://doi.org/10.1001/archpedi.162.8.712
Weernink, M. G., van Wijk, R. M., Groothuis-Oudshoorn, C. G., Lanting, C. I., Grant, C. C., van Vlimmeren, L. A., & Boere-Boonekamp, M. M. (2016). Insufficient vitamin D supplement use during pregnancy and early childhood: a risk factor for positional skull deformation. Maternal & child nutrition, 12(1), 177–188. https://doi.org/10.1111/mcn.12153
Williams, E., Galea, M. (2023). Another look at “tummy time” for primary plagiocephaly prevention and motor development. Infant Behavior and Development 71, Article 101839. https://doi.org/10.1016/j.infbeh.2023.101839
World Health Organization (n.d.) Head Growth Charts. Retrieved August 1, 2023, from https://www.who.int/tools/child-growth-standards/standards/head-circumference-for-age
World Health Organization (n.d) Head circumference-for-age GIRLS: Birth to 2 years. Retrieved August 1, 2023, from https://cdn.who.int/media/docs/default-source/child-growth/child-growth-standards/indicators/head-circumference-for-age/cht_hcfa_girls_p_0_2.pdf?sfvrsn=471935f4_13

How’s your sense of smell? 7 things you may not know about OLFACTION.
By Aromatherapist and Massage Therapist, Sonya Edmonds As an aromatherapist I find olfaction – smell – fascinating, and it’s always at the forefront of my…